
Hello everyone!
I’m happy to see a storm in the forecast, and I’m sure you must be as well. In this med ed email, I’m introducing a new recurring section in which I’ll review a small piece of pertinent anatomy— something that we often encounter or hear about from our patients when they reach the hospital.
Meeting with Bend Fire Chief, Jan 30.
DT, Stonich, and I had a good meeting with one of the deputy chiefs from Bend fire, along with Bryce Campbell PA from the mountain clinic. The goal was to make sure we’re working together well and keeping any issues out in the open. It was a productive meeting (eg. they didn’t have a good phone number for dispatch!) and I’m happy to say that I think we’re working well together. They had the opportunity to see our side of things in action, as there was a Code 3 head transport in progress while they were there.
As an example of things working well, of all of the ground ambulances requested this season (17-18 so far) only one has resulted in a non-transport, which suggests that we’re doing a great job of triaging our patients and using EMS appropriately. Keep up the good work!
We brought to their attention that crews coming up will sometimes ask questions that can imply that they think a transport could be avoided (“does this patient have someone who can give them a ride to the hospital?”). While it’s appropriate for crews to call and ask for patient updates, they shouldn’t be trying to talk us into a refusal. If you encounter this, don’t push back, just stick to giving an update and let them decide with the patient whether to transport. Please inform Stonich or I of any similar cases that you encounter so we can keep tabs on the issue.
New Patrol Case
Back for 2026 is a new patrol case! This one is a doozie of a sick patient. I won’t ruin the punch line, but the title is a clue. Take a run through the case when you have a slow hour on a cloud bump.
As always, you can find a link to the patrol cases table of contents at the bottom of the protocol page, Patroller.Ski
Anatomy Nug: Acetabulum
A skier falls on their side in the park or a pedestrian slips on ice. Both land on their side and complain of hip pain. There’s no deformity, but they can’t walk and are taken by ambulance to hospital where they’re diagnosed with an acetabular fracture.
The acetabulum is the pelvis side of the hip joint. As I learned recently from one of you, it means “little dish” in Latin, That makes sense, as it’s the dish shaped portion of the pelvis that the femoral head sits in. It sits at the junction of the three main pelvic bones, the ilium, ischium, and pubis.
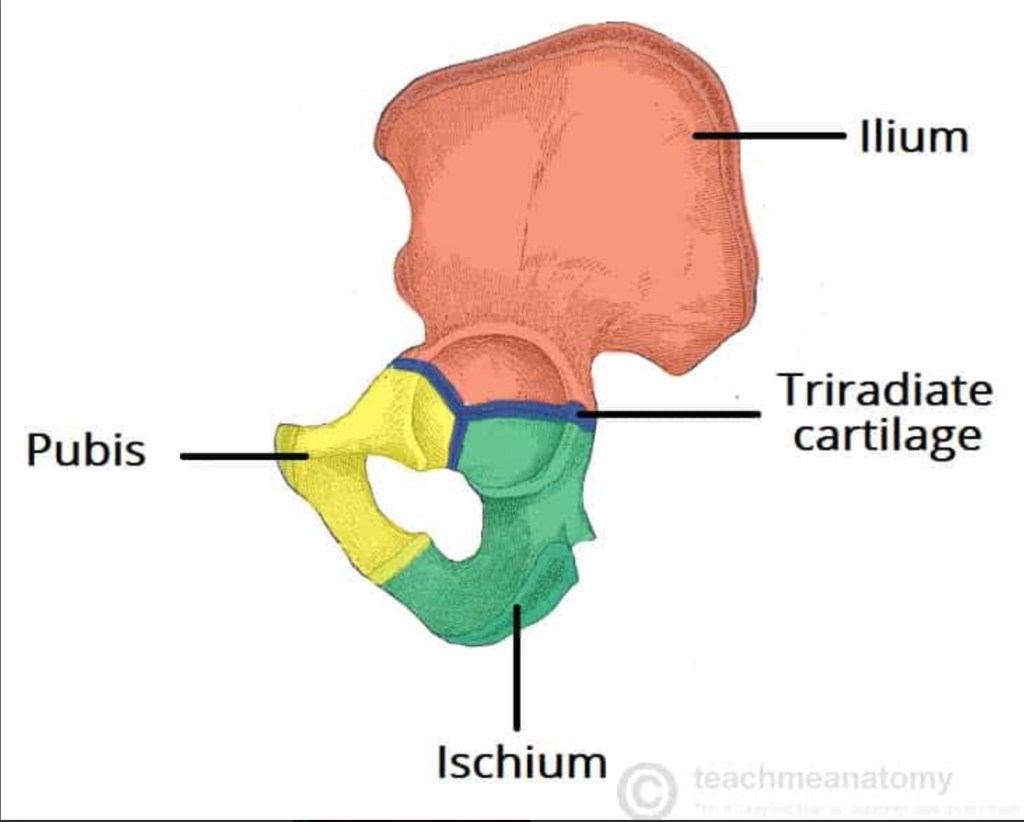
The cartilage shown here is present in kids but the bones fuse and adults have no cartilage.
Fractures of the acetabulum can often be managed without surgery if they’re not displaced, meaning that all of the bones are in alignment. Essentially, if it’s just a crack in the bone, the patient can bear weight as tolerated and usually goes home with crutches and pain meds. Any displacement, however, causes unevenness in the joint surface (articulate surface) of the acetabulum, and can cause terrible pain and arthritis of the hip if it’s not realigned surgically.

This 3d CT scan reconstruction shows the ball of the femur punching through the anterior wall of the acetabulum, and multiple bone fragments. This displaced fracture is going to need surgery.
That’s it for this med-ed email. As always, shoot me your feedback or questions by text, or reply to this email. Keep up the good work. What you do matters!
-PF
