

A thought from Shane Parrish at Farnam Street Blog:
“Talent and potential mean nothing if you can’t consistently do the boring things when you don’t feel like doing them.”
And from Sun Tzu, The Art of War:
“Tactics without strategy is the noise before defeat.”
This educational email is the first of a multipart series on the basics of airway management. This is a core skill for any BLS provider, and it’s a critical skill at all levels of practice. We physicians in the trauma bay use the same principles and approach. The beginning of the algorithm is the same, we just have a deeper tool chest.
This first education email will focus on the physiology (what’s the point of breathing?) and the anatomy. This is important knowledge because it allows us to understand why we do what we do when managing an airway.
What will follow are my recommended airway management roadmap, and the microskills that you should have deeply engrained to be able to execute under stress.
Physiology
Respiration
Respiration refers to the process of exchanging gas with the environment. As we inhale, we are bringing in a fresh supply of oxygen, and as we exhale, we are getting rid of excess carbon dioxide.
Inhaled air is 21% oxygen at both sea level and at altitude. However, the partial pressure of oxygen at sea level is 160 mmHg, while at 7000′ it’s only 125 mmHg, which is functionally about 20-25% less.
Exchange/adsorption of oxygen in the lungs is extremely fast and efficient. This means that effective oxygenation of the blood can be accomplished even if a significant fraction of the lung tissue isn’t in the game. As an example, people do OK after having one of their two lungs removed.
In contrast, getting rid of CO2 is slower and more dependent on the volume of lung that is being used for respiration. Practically speaking, this means that to improve oxygenation in patient, we should improve the fraction of inspired oxygen (give them oxygen!). Giving them breaths faster doesn’t help. In contrast, when CO2 is the issue, increasing respiratory rate and respiratory volume is the way to fix the problem. For most medical emergencies encountered on the ski hill, oxygen delivery is the issue, even in something like an asthma attack.
Respiratory Drive / Apnea
Take a deep breath. Hold it. Feel the increasing urge to take another breath. That’s your respiratory drive (you can breathe out now).
In most humans, the respiratory drive comes from the brain stem sensing the concentration of CO2 in the blood, which increases pretty quickly when you stop breathing. Some people who have chronically elevated CO2 levels (emphysema/COPD) will have a respiratory drive that’s based on oxygen concentration, but these folks are going to be very rare in our ski population.
In contrast to rapidly rising CO2 levels, oxygen (O2) levels in the blood decrease more slowly. A volunteer who has breathed 100% O2 for several full breaths before being paralyzed will have a pretty normal oxygen concentration for 6-8 minutes without breathing. Without preoxygenation, a person who stops breathing (apnea) will maintain a normal oxygen saturation for 2-4 minutes before oxygen drops rapidly.
Elevated CO2 levels in the blood can cause fatigue, confusion, and altered mental status, but CO2 alone is rarely a fatal problem. In contrast, low oxygen levels are tolerated for only a few minutes before cardiac arrythmias emerge and brain tissue starts dying. Accordingly, most of our efforts in managing the airway of critical patient are focused on delivering high flow oxygen as soon as possible before the brain and heart start to flag.
Anatomy Nugget: The Oropharynx
Oro-pharynx is a fancy way of saying mouth-throat. The term refers to the terrain that begins at the teeth/nostrils on down to the vocal cords. Refer to my highly technical drawing for more details:
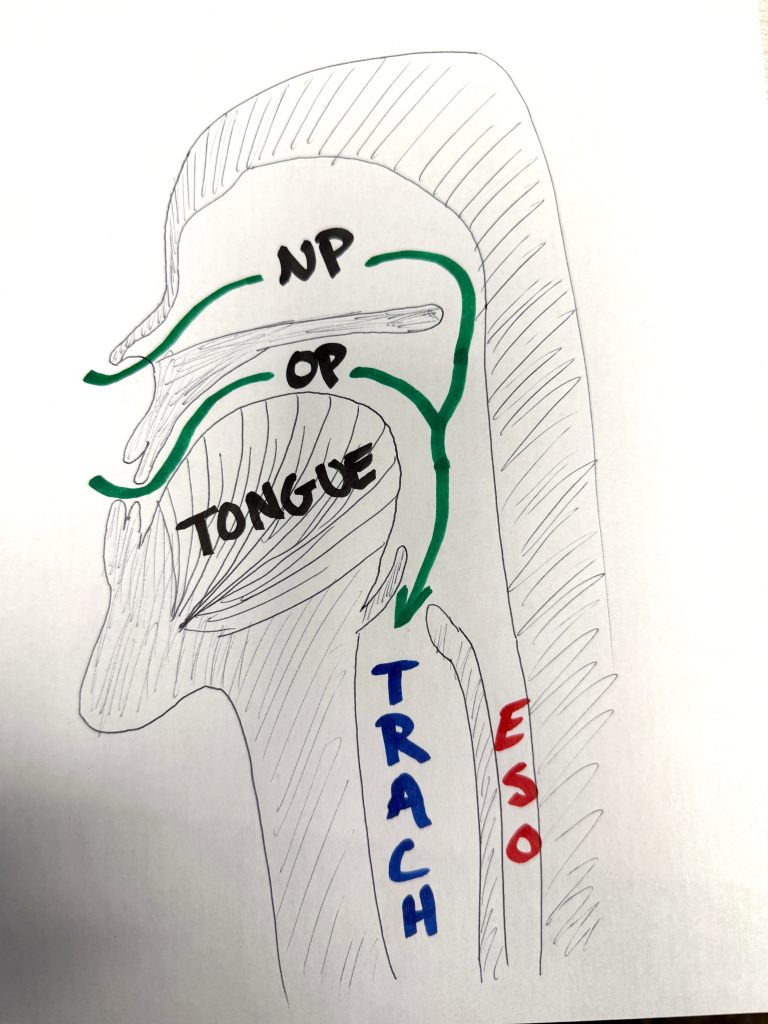
NP: Nasopharynx; OP: Oropharynx; TRACH: trachea; ESO: esophagus.
The point to take away from this picasso is that there are two ways to deliver air flow to the trachea (windpipe), either through the nose or the through the mouth. The tongue here is basically to scale: it’s enormous, and has a nasty habit of getting in the way of attempts to ventilate through the mouth. Also worthy of note: any airflow delivered through either the nose or the mouth is directed at both the trachea and esophagus until an iGel LMA or more advanced airway is in place.
Take Aways:
- Oxygen delivery is usually our primary concern, and apnea leads to problematic hypoxia in 2-4 minutes.
- Improved O2 delivery is best achieved by increasing the fraction of inspired oxygen (eg. NRB), not by breathing the patient faster or deeper.
- Both the nose and the mouth work for delivering airflow to the trachea, but the nasal route avoids the enemy of airway management, the tongue.
- Until an advanced airway is in place, any breaths delivered will hit both the trachea and the esophagus.
Up Next
You can look forward to a review of available airway management tools and how I think about moving through an airway management algorithm for our patients.
Until then,
P
