

Holy heck, welcome to spring! It was quite a day of skiing yesterday and the mountain is getting hot and sunny today. I hope that you were all able to ski some well-deserved powder.
End of Season Review
I hope that available pro patrollers will join us next Friday April 10th, 5:30 pm at Embark Coworking. We’ll be reviewing some of the significant cases from the year and I’ll be giving a talk on traumatic cardiac arrest and neurogenic shock.
Your Professionalism is Awesome
I want you all to know that I have gotten several comments from ski clinic staff, Mt Bachelor staff, and members of the public expressing their gratitude and admiration for the professionalism that you display every day. You’re doing an awesome job of showing up to calls with great attitude, compassion, and showing that you care. Keep up the good work and know that it’s being appreciated.
Med Ed: Airway Tools
Last time that I was in the clinic I tried to make an airway trainer head available to do some hands-on work with a few of our usual tools. The universe didn’t agree with my plans that day, so I made a video that walks through the basic airway tools and some small tips or tactics that might be useful with each of those. I’ll list out some of the high points below, but I’d encourage you to take a look when you have the time and send any questions or comments that you might have.
Basic Airway Tools for Prehospital and Ski Patrol Use
Pocket Mask
- Make sure to expand the mask. They pack flat. Pop it out before using.
- The narrow end goes towards the nose.
- Yours should have a one-way valve on it to prevent your patient from vomiting into your mouth. If it doesn’t seek one out.
- Where the valve connects is a different diameter than that of the BVM. If you switch to a BVM, use the mask that comes with the BVM.
- Pull the patient’s face/jaw up into the mask before giving breaths, don’t smush the mask down onto the patient’s face.
NPA
- Airway adjunct to make ventilations easier. Useful in unresponsive as well as less responsive patients.
- Measure from the philtrum of the nose (where a bull has it’s ring) to the tragus of the ear. This is the firm cartilage right in front of the ear canal opening.
- Look into the nose and decide which nostril looks bigger. Use that one first.
- If needed, you can double barrel, NPA on both sides.
- Insert straight back along the floor of the nose, not upwards. Straight back level with the ear lobe, not upwards at the same angle as the bridge of the nose.
- If you meet more than very minor resistance, try the other side or downsize, don’t force it.
- Lubricate well.
- Don’t use an NPA if: significant nasal trauma or trauma to the roof of the mouth, suspected skull fracture (black eyes, unstable facial bones, bruising behind the ears, bleeding from the ears. Why? It’s bad form to place an NPA into the brain.
OPA
- Adjunct to assist with ventilations, useful only in unresponsive patients who don’t gag with insertion.
- If the patient fights placement, remove the OPA. Triggering a gag can cause vomiting and aspiration.
- Helps in 3 ways: 1) Pulls the tongue off the back of the mouth, 2) provides a direct straw-like channel to the back of the mouth, 3) acts as a bite block that keeps the patient from clenching closed.
- Measure from the earlobe to the corner of the mouth. Better that the OPA is too big than too small. For some reason the one that fits most adults is often colored red.
- Textbook insertion: point the tip of the OPA to the roof of the mouth then flip around when halfway in to match the curve to the tongue.
- My preferred tactic: used a gloved hand to open the mouth and hook downwards on the tongue, making space. Insert the OPA into the mouth either sideways or matching the curve of the tongue.
- Big big tongue? Use a piece of gauze to grip the tongue and pull it forward out of the mouth, then insert.
- Contraindications: gagging or alert, severe facial trauma, foreign body in the back of the mouth/airway.
BVM
- Used to provide ventilations through a mask or LMA (see below)
- Best used with supplemental oxygen attached, can be used with room air.
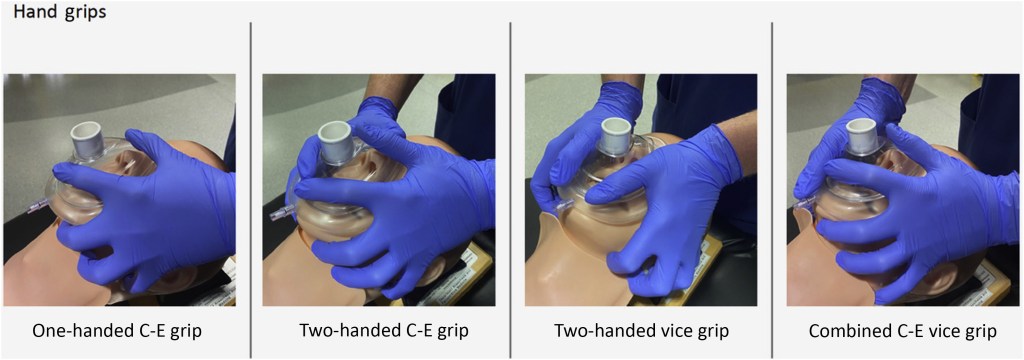
- One-person BMV use is very difficult. If resources are available, use 2 person technique. Person 1: Provides a 2-handed mask seal, pulling the face up into the mask. Person 2: Provides ventilations by squeezing the bag.
- Squeeze the bag gently, don’t flatten it. Observe chest rise then stop. Excessive bagging inflates the stomach.
- If you have to provide BVM ventilation as a single rescuer, used the C-E hand technique for mask grip. Try this on Bad Jerry and tell me it isn’t darn hard.
- The BVM doesn’t fit onto a pocket mask, so make sure to use the mask that comes with the BVM.
- It does fit onto the LMA/iGel.
iGel/LMA
- ALS advanced airway tool, used to deliver ventilations more directly to the vocal chords/trachea, and to try to keep any vomitus or secretion from going into the trachea.
- We use the iGel which is a type of Larygeal Mask Airway (LMA). These are great because they’re simple and don’t have any moving or inflatable parts like some other LMAs.
- Like an OPA, the LMA is appropriate only for unresponsive patients who tolerate its placement without gagging.
- There are a range of sizes. For iGel, the green one fits most adults. There is a weight-based sizing on the small box it comes in. Orange color for big humans, yellow color for slightly smaller humans.
- Keep the box handy. Prior to insertion, lubricate well and then rest in the box.
- Place the green retention strap behind the patient’s head to have it ready.
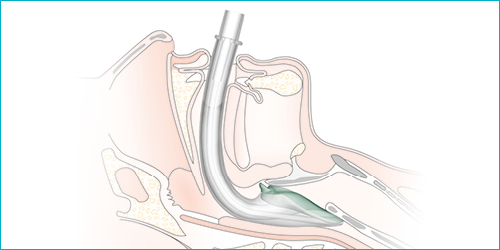
- To insert, jaw thrust or hook the tongue as per the OPA to make space, and insert along the curve of the tongue. Seat firmly into the back of the throat. Then secure with the elastic strap. Full procedure here.
- If you hear air coming from around the igel when ventilating: 1) Gently reseat the iGel into the back of the throat. If that doesn’t work, consider moving to a larger size.
- If you can’t ventilate through the iGel, it is probably too big. Downsize.
My Prehospital Airway Plan
Every situation is different. This isn’t a protocol, it’s just the plan that I have in my head for how I will march through my airway tools on a patient with inadequate respirations.
- Arrive to patient who is minimally responsive: assess for pulse and respirations.
- If respirations are inadequate: ensure no foreign bodies in the mouth, perform a strong jaw thrust, reevaluate.
- If still inadequate, use pocket mask to assist with ventilations. Give a few breaths, then improve using additional tools:
- Place NPA +/- OPA if tolerated. Resume ventilating using mask.
- When additional resources arrive, ventilate using BMV over the NPA/OPA. Use 2- person technique.
- When ALS arrives, if patient remains unresponsive, remove OPA, place LMA/iGel. Leave NPA in place as future backup.
- Ventilate through the LMA using the BVM.
Wrap Up
Thanks as always for your interest and the excellent care that you deliver. Please let me know if you have any questions or other topics that you’d like me to address!
-Patrick
